AV Heart Block
Atrioventricular (AV) block occurs when atrial depolarizations fail to reach the ventricles or when atrial depolarization is conducted with a delay. Three degrees of AV block are recognized.
First-degree AV block consists of prolongation of the PR interval on the electrocardiogram (ECG) (> 200 msec in adults and > 160 msec in young children). The upper limit of the reference range for the PR interval is age-dependent in children. All atrial impulses reach the ventricles in first-degree AV block; however, conduction is delayed within the AV node (see the image below).

First-degree atrioventricular block. PR interval is constant and is 280 msec.
Second-degree AV block is characterized by atrial impulses (generally occurring at a regular rate) that fail to conduct to the ventricles in 1 of the following 4 ways.
The first form of second-degree AV block is Mobitz I second-degree AV block (Wenckebach block), which consists of progressive prolongation of the PR interval with the subsequent occurrence of a single nonconducted P wave that results in a pause. The pause is shorter than the sum of any 2 consecutive conducted beats (R-R interval).
An episode of Mobitz I AV block usually consists of 3-5 beats, with a ratio of nonconducted to conducted beats of 4:3, 3:2, and so forth (see the image below). The block is generally in the AV node but can occasionally occur in the His-Purkinje system and is termed intrahisian or infrahisian Wenckebach (depending if the block occurs within or below the His-Purkinje system).
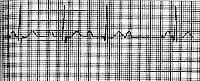
Second-degree atrioventricular block, Mobitz type I (Wenckebach). Note the prolongation of the PR interval preceding the dropped beat and the shortened PR interval following the dropped beat.
The second form is Mobitz II second-degree AV block, which is characterized by a constant PR interval followed by sudden failure of a P wave to be conducted to the ventricles, so that either an occasional dropped P wave or a regular conduction pattern of 2:1 (2 conducted and 1 blocked), 3:1 (3 conducted and 1 blocked), and so on is observed (see the image below).
Second-degree atrioventricular block, Mobitz type II. A constant PR interval in conducted beats is present. Intraventricular conduction delay also is present.
The third form is high-grade AV block, which consists of multiple P waves in a row that should conduct, but do not. The conduction ratio can be 3:1 or higher, and the PR interval of conducted beats is constant. This is a distinct form of complete AV block, in that the P waves that conduct to the QRS complexes occur at fixed intervals. For complete AV block, no relationship exists between the P waves and QRS complexes.
The fourth form is 2:1 AV block. This could be either Mobitz I or Mobitz II, but distinguishing one variety from the other is nearly impossible.
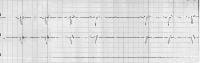
Third-degree AV block is diagnosed when no supraventricular impulses are conducted to the ventricles. P waves on the rhythm strip reflect a sinus node rhythm independent from QRS wave complexes. The QRS complexes represent an escape rhythm, either junctional or ventricular. The escape rhythm originating from the junctional or high septal region is characterized by narrow QRS complexes at a rate of 40-50 beats/min, whereas escape rhythm from low ventricular sites is characterized by broad QRS complexes at a rate of 30-40 beats/min.
No relationship exists between the rhythm of P waves and the rhythm of QRS complexes in third-degree AV block. The frequency of P waves (atrial rate) is higher than the frequency of QRS complexes (ventricular rate) (see the image below).

Third-degree atrioventricular block (complete heart block). The atrial rate is faster than the ventricular rate, and no association exists between the atrial and ventricular activity.
AV dissociation is a rhythm identified by atrial and ventricular activation occurring from different pacemakers. AV dissociation does not indicate the presence of AV block and is distinctly different. Ventricular activation may be from either junctional pacemakers or infranodal.
AV dissociation can occur in the presence of intact AV conduction, especially when rates of the pacemaker, either junctional or ventricular, exceed the atrial rate. Third-degree AV block can occur with AV dissociation. However, in AV dissociation without AV block, the ventricular rate can exceed the atrial rate and conduction can occasionally occur dependent on the timing between the P wave and the QRS complex.
AV block may also occur in patients with atrial fibrillation (see the Atrial Fibrillation Center). Regular R-R intervals are possible in the presence of AV block (generally at slow regular rates).
No comments:
Post a Comment